(My actual homemade EMR created with Pages program on my MacBook Pro laptop!)
With so many doctors bitching about electronic medical records, I just want to scream from the mountaintops, “I LOVE my EMR!” And you can love yours too! As you all know, I created my own DIY EMR back in 2005 and I’ve never spent a dime on it. Zero. I already owned my laptop and I’ll share more about the whole adventure shortly so you can replicate it if you like.
Disgusted with assembly-line medicine, I literally had to get out of the big-box clinics to save my life. My job made me suicidal as you know. So I held a series of town hall meetings where I invited my community to design the ideal medical clinic—and we launched in April 2005. I’ve been living the happily-ever-after life ever since. Part of having an ideal clinic is having an ideal medical record system. I’ve helped hundreds of docs launch ideal clinics an find ideal medical record systems so I know you can do it too!
Need help designing your medical record system? Contact Dr. Wible here.
People have been begging me for years to describe how I created my DIY EMR (Do It Yourself Electronic Medical Record) so finally I’m sharing the whole darn thing on a live call with you all (and I’ll be posting the first half of our call on my blog so I can demo my EMR for all the docs out there who aren’t with us tonight). I literally was so insanely excited about our medical records happy hour tonight, I could barely sleep! Seriously. Who else is as excited as me about medical record keeping? I must be a total geek.
So in case you missed our first call (part of our “I LOVE my EMR” month!) here it is: How to fall in love with your EMR—a journey through the magical and mysterious history of our doctors’ transition from 3-by-5 index cards to electronic medical records. Beyond fascinating!
Let’s review the 3 main functions of medical records.
1) Medical record of patient progress (primarily for patient)
2) Documentation for insurance billing/coding (primarily for you)
3) Legal protection in case of lawsuit ( primarily to protect you)
Notice only ONE of these has anything to do with the patient. Let’s break this down a bit more.
1) Medical record progress note documents the medical progress of your patient and you will be happiest and in the most congruent state for healing and most likely to create a true therapeutic relationship if you remain attentive to the patient’s needs (not billing/coding and potential lawsuits).
2) Documentation for insurance billing/coding has nothing to do with the patient—and is a huge distraction to patient care. If you have a cash-based or DPC practice you can debulk the chart note by at least 50%. Maybe even write one-liners like, “Splinter removed. Patient happy!’ You don’t need to click boxes that make no sense and complete a full review of systems just to meet coding criteria. YOU ARE LIBERATED. Even if you do choose to accept insurance, you can utilize very straightforward templates that you can create (either paper or electronic) plus you can code by TIME spent with patient—to further debulk your chart note while getting paid for your time and expertise. I encourage you to maximally DEBULK your chart notes so you can recoup your time. TIME is what builds the therapeutic RELATIONSHIP.
NOTE: Physician fear of over/undercoding creates a near-obsessive tendency to spend way more time on the chart note than is necessary. Why? Physicians and other health professionals spend their lives in extreme fear of being audited and it rarely happens!!! Think about it: 1) You are small beans compared to high-dollar high-volume procedure-based practices in assembly-line clinics. 2) Audits are primarily generated by Medicare (so if you don’t accept Medicare you are pretty much home free), Medicare audits can go back up to 3 years. So you are definitely home free if you’ve opted out more than 3 years ago! I know only one doc who has ever been audited by Medicare and he’s in anesthesia (Medicare audited ALL independent anesthesiologists in his state—and he owed like 1 million dollars). The only other audit I personally know about was Karen Smith. Please see my blog I love old people, but I will not accept Medicare to view the horrific video of what happened during her Medicare audit. 3) The only time I’ve been asked for a chart note in 14 years has been by a car insurance company post patient motor vehicle accidents! NEVER BEEN AUDITED. If you don’t accept insurance, it is impossible to get audited. If you don’t accept Medicare (but take commercial insurance) you are extremely low risk. Stop worrying about it already!
3) Legal protection for medical liability is also a huge distraction. By the way avoid the word MALPRACTICE (the word already assumes you are guilty! Way better to call it medical liability insurance vs. office liability insurance which is insurance for slip and fall—often included in your medical liability insurance policy so don’t make the mistake I did early on and double pay another company!) You are at the lowest risk of your career in an ideal clinic. Remember the difference between production-driven vs. relationship-driven care. It is the relationship that safeguards you from liability—even if you have a bad outcome.
Example: Recent risk-reduction class I attended (for which I save 3% annually on my medical liability premium) the following case was shared: Lady had bad outcome during hospitalization. She went to an attorney who reviewed her medical records and pulled every single doctor on the chart. Before dragging them into court, he shared the doctors’ names with the patient. She agreed that they should all be brought into the lawsuit “except this one” she said. “This is my family doctor. I like her.” Even if you do something wrong, patients do not generally sue someone they like.
NOTE: Reasons why you are at the lowest medical liability of your lifetime: 1) You are in a relationship-driven ideal clinic. Patients with good relationships with doctors, don’t sue them. 2) You offer 30-60 minute visits (not 7 minute) so better medical decision-making prevents errors. 3) Your patients can finally trust you. As you recall from our prior session on EMR (see How to fall in love with your EMR) you will be able to overcome the culture if distrust that pervades the typical assembly-line visit. Patients now have time to reveal their REAL TRUE LIFE to you!!! Especially if you have paper charts or are not on the cloud or in some large EMR system (some patients are super suspicious of these larger systems).
5 ways distrust undermines medical records (see How to fall in love with your EMR)
Fear of discrimination makes comprehensive medical records a joke due to 1) Pre-existing-condition discrimination. 2) Drug discrimination. Due to federal government’s inclusion of marijuana as an illegal schedule 1 narcotic, even suggesting CBD oil can be seen as violation of regulations. 3) Sexual-orientation discrimination. Lesbian, sex worker, polyamorous relationships not declared to doctors leading to obvious difficulty is screening/risk reduction conversations and exams. 4) Mental-health discrimination. Physicians/veterans/firefighters/paramedics mental health disclosures may lead to employment discrimination. Also professional athletes. VIP types. pilots. Ongoing fear of denied benefits based on mental health diagnoses. 5) Legal-system discrimination when medical records release to attorneys during divorce, criminal, civil and child custody proceedings Workers compensation attorneys deny claims based on previous alcohol use or drug experimentation.
To recap: 3 main functions of medical records.
1) Medical record of patient progress (primarily for patient)
2) Documentation for insurance billing/coding (primarily for you)
3) Legal protection in case of lawsuit ( primarily to protect you)
Given the most progressive practice is one that is truly patient-centered, I am encouraging you to have a patient-centered medical record . Most ideal clinics can return to the truly patient-centered medical record.
Now that we have returned to the original primary intention of the medical record, let’s use it properly—and have FUN! Here are my 5 tips and then I’ll share how I created my own perfect-for-me-and-my-patients homemade EMR.
1) Create a medical record that allows you to ENJOY your visits! Is there a question you want to ask that is not on the “official” EMR? Then create your own unique and ideal medical record. You can use paper charts, index cards, electronic. Yes, it IS legal. (All commercial insurance allows you to use whatever system you like. Only Medicare has the meaningful use crap—and just eat the 2% penalty or whatever rather than jump through all the hoops is my best advice).
2) Create an ideal intake that is a barrier/obstacle for non-ideal patients, and a welcome mat for ideal patients. Weed out non-ideal from ideal. No guilt. Your non-ideal patient is someone else’s ideal patient. Trust me. There are enough patients for everyone. No need for turf wars. Geez. Offload intake work to patients and they complete all in advance of visit.
3) Complete chart notes while WITH patient during the 30-60 minute visit. NOT AFTER. Some of you are organizationally challenged ADHD overthinkers and you must stop overcomplicating your lives.
Offload work to patients. Do prior authorizations in real time during office visits. Avoid all stray work between visits.
4) Debulk your chart notes. Yes, you need to perform surgical debulking on your entire medical record system. See how few words you can use to get the essentials in the chart. Stop writing mini novellas for each visit. Nobody wants to read an 8-page note about an ingrown toenail. Just stop already!
5) Experiment with streamlining charting even further. Hey, consider writing chart note ahead of the visit! That’s something that I did for a while. I cut and pasted in patient emails and carried over some of the issues I wanted to follow-up on from last office visit. Drag and drop templates for physicals. I would have half the chart note done before patient even arrived. Literally I only had a few things to add. Oh, and by the way I did this in a coffee shop every morning (see photo at top). SO MUCH FUN!!!!
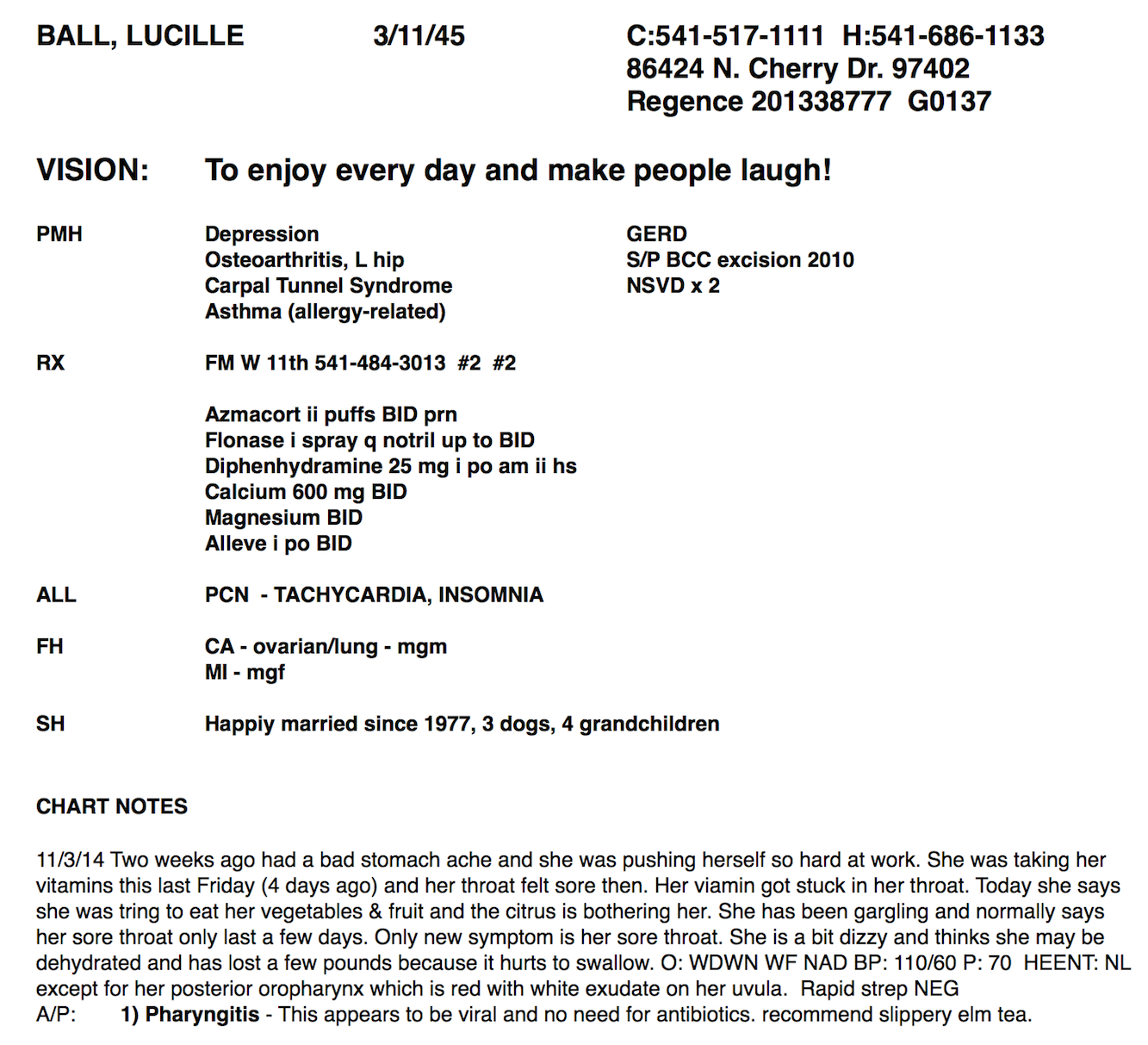
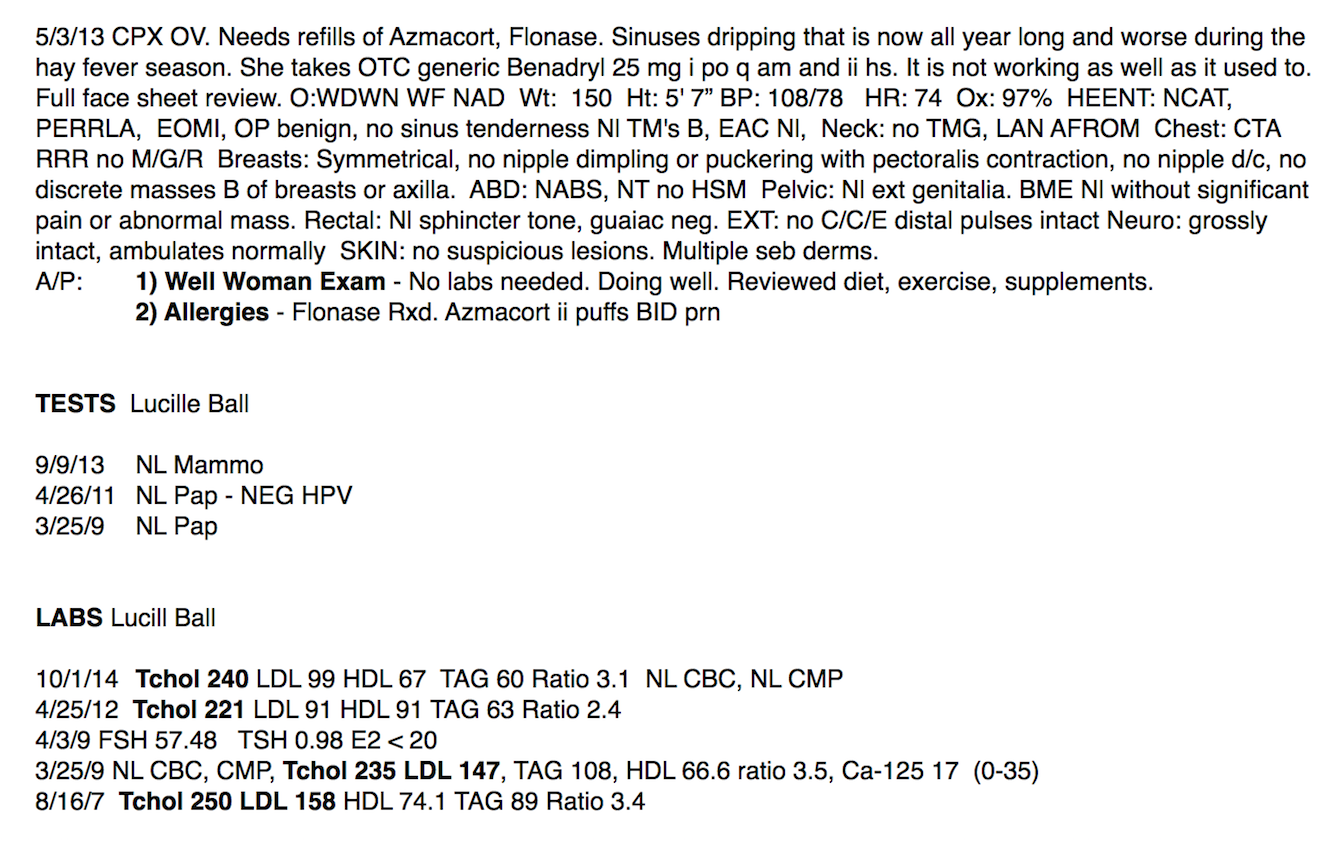
Now check out the two screenshots of a sample chart note on my favorite patient. Notice that I start with a bold face sheet with essentials (and I bold all significant abnormals and diagnoses in progress notes so I can easily scan ONE scrolling window for what I need to know quickly). I begin with a VISION STATEMENT so I can keep my patient’s ultimate goals top of mind. In one scrolling document I have everything with most recent chart note first and all labs/tests at the bottom. So freaking simple! If you need help designing your medical record system, contact Dr. Wible here.
Now YOU try it. What would your cool homemade EMR look like?
Need help? Contact me. I’m happy to help you!











Lovely! Btw, I don’t think the “how can one person do all this?” comment is a criticism, more like awe. I’ve been out of medicine for a year and am continually amazed by the reflexive quibbling that goes on in medicine, which I didn’t really notice when I was drinking the Koolaid. I suspect these are the people who got picked on in school for having an adverse personality. I do think there might be a point about cultural appropriation, though. If nothing else, it’s distracting from your major message. I am sending your article to a fourth year med student who is going into the air force to pay back loans, to keep her aware that there is light at the end of the military commitment tunnel.
Advantages of home made EMR have been outlined. Audit points have been explained but more discussion on insurance would be preferable. Thanks for posting.
Hello!
I wanted to ask about something I did not see mentioned, something that providers need to consider; Securing patient data (at rest and in motion.)
What steps do you take to protect patient PHI/PII from unauthorized access?
Do you utilize industry standard security practices such as robust data encryption?
Audits and liablity aside, patient record compromise due to unsecured data or improperly configured security measures directly harms patients and far overshadows any concerns about the use of “larger EMR systems”.
Best to avoid HHS’ “Wall of Shame”
My partner is an IT guy and assures me I have some of the most secure records in the country. Password protected. Data encrypted. Off the cloud. . . no staff in my office and inaccessible to anyone in the world except me. VERY very secure.
Looking at starting a cash clinic in my area due to high number of uninsured folks. Came across your page through the suggestion of a fellow alumni from Frontier (I’m a FNP).
Love your site, thank you for the effort I know it takes to put this all together and maintaining it. But most of all thank you for sharing your knowledge and expertise.
Ed
I agree completely with the author. During pandemic times, it became more common to receive treatment online rather than at a hospital. I think innovative health care must be connected to modern strategies, which are obvious good ideas. Good job!
The entire process of work and data collection is described in detail and point by point in the article. Thanks! I would like to know more about insurance, but maybe next time.
Hello Dr. Wible. Are you able to ePrescribe? What about Eprescribing controlled meds?
Yes I can and the rules vary state by state so check with your state regulators/med board.
Thank you for a really interesting and relevant topic.
How do you e-prescribe.
This is excellent Pamela.
Thank you for showing everyone how to stop the fear of practicing
This beloved profession according to the OATH we all took.
You can add on iPrescribe (or other platforms) though they will not be integrated with my self-made EMR. If you are techy you may be able to integrate somehow. I LOVE my EMR 🙂
Oooooh and the coll thing about my new coaching practice (retired my medical clinic after 30 years) IS . . . I earn more and no longer need to chart at all!!!! Let me know if you are ever interested in that. More here: Launch your coaching practice—without a medical license https://www.idealmedicalcare.org/launch-your-coaching-practice-without-a-medical-license/
INTERESTED IN DIY EMR. ARE YOU PLANNING IN GROUP SESSION IN THE FUTURE TO DISCUSS?
We’ve had several in the past. Happy to have a private session to walk you through the process. I LOVED my DIY EMR.