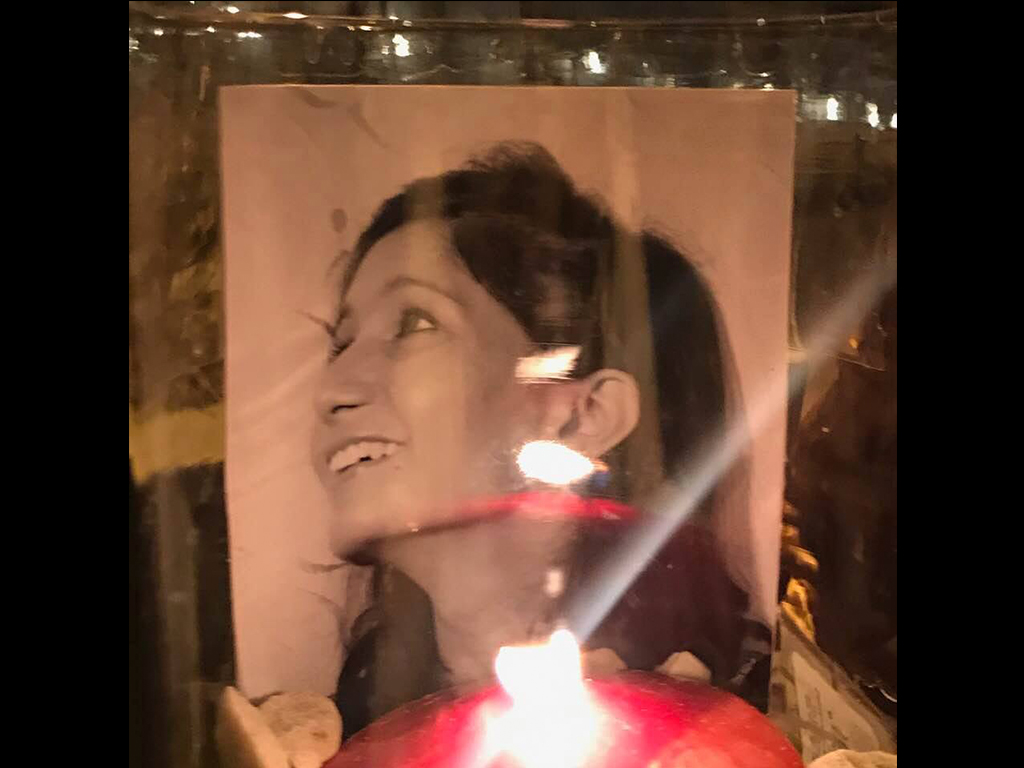
Tonight we gather as a community. Each of us to shine our light on the most recent suicide. On the life of a brilliant, loving, kind woman. A woman who dedicated her very life to helping and healing others. As a doctor.
Dr. Deelshad Joomun was not just a doctor. She was one of the first interventional nephrology fellows—and more importantly the first female one. It was not an easy road and she carved her path largely on her own reaching the pinnacle of success. Yet one week ago standing in her white coat on the roof of this 33-story building housing hundreds of hardworking doctors from Mount Sinai hospital, she stepped off the ledge.
Tonight we stand on the ground where her heart stopped. To celebrate Deelshad. Her very name means “happy heart.” An idealist, an inspiration to all, humble despite her massive success, she was never one for the limelight. Yet her life and death must not remain in the shadows.
Though first in her field, she is not the first doctor suicide at Sinai. In less than two years, three brilliant young women leapt to their deaths. Two right here.
As we pay our respects to all three—to Esha, to Kathryn, and to Deel—we also shine our lights on all the invisible ones. The hundreds of thousands of doctors who have gone before them. I was almost one of them. Though I survived, I’ve lost countless colleagues to suicide.
To heal it will take courage and community
Courage means to lead with one’s heart. And we must each have courage. Courage to stop blaming the victims as sad and weak. Courage to do more than just send another “tragic loss” email. Courage to confront institutional censorship and intimidation. Courage to fully investigate each of these suicides.
And so we gather and grieve as a community—not just Mount Sinai. Not just New York City. More than one million Americans lose their doctors to suicide each year. This is also a global public health crisis. Many die a direct result of their training—institutionalized cruelty with rampant human rights violations illegal in any other industry.
I’ve written about Deel’s suicide. Now with 20,000 Facebook shares. These flowers have been sent here from grieving people from all across the country and the world. And we must grieve as a community because the loss is far reaching. These suicides can no longer be hidden in a private funeral for the family.
Now the world is watching.
Nearly 500 residents in this building—neighbors and her friends—saw her dead body outside their windows. People on the sidewalk who screamed and called 911. The building super, the man at the concierge desk who knew her. Sinai staff and nurses now whispering in hallways (all told to keep quiet, not speak to reporters). And the thousands of patients she cared for now wondering what happened to their beloved doctor. They all must be allowed to grieve with us.
And there is another group that is watching—the depressed and suicidal doctors from all over the world who are living with the same agony. They are on the ledge now. Doctors who write begging me for help because they “don’t want to be the next one under the tarp.”
We can no longer cover up our doctor suicide crisis with a tarp and silence. We can no longer discard our doctors into body bags without investigation. We must all stand up for our brothers and sisters in medicine who walk into our hospitals and clinics everyday to so selflessly serve others.
May Deelshad rest in eternal peace and love.


Previous articles on her suicide: Suicided doctor: covered with a tarp—and silence. Also on KevinMD. Doctor suicide: where are the vigils, cards & flowers? Refinery29 reports This hospital has a physician suicide problem.













It’s obviously hard. And yet this awful suicide must be acknowledged. We must care. Doctors are the resource. We must care for them.
It just seems a shame to me that good doctors have to DIE to get anyone to pay attention to one of the most disturbing by-products of “corporate medicine”/”managed care”.
The cold/calculated/often brutal systemic abuse of physicians – particularly of women – just to make an extra buck – or secure a “suit’s” bonus.
And ever more shocking is how few people really care. And the near complete lack of media coverage.
corporate medicine, okay, but not managed care. Henry Kaiser began his system in the Central Valley San Joaquin Valley of California in the ’40s to bring some semblance of health care to the migrant Mexican workers in the fields. He was pooh-poohed for the next 30y+. Around that time, out of self-imposed isolationism and into post-WWII basking in the glory of globe trotting leaders (vs domino theory vacuum theory of USSR/Red China/NK, business and government came together and entwined together jobs and health care. The medical system learned rapidly the sum of the parts are worth more than the whole. By the early ’80s the renamed capitated system and private insurance roared back and took control throttling those up and coming medical servers who had been feeding at the hole of prestige nobility wealth adoration, all false. the older docs had made it, yay, while those new young fools dreaming of pedestals found security in a 9-5 job and various acronyms of physician groups, i.e. IPAs etc. and science grew and research and knowledge bases and demands and cut-throat practices to colleagues and to those coming up new into the system. There was and there remains a god-wish amongst physicians and particularly sturgeons. As usual women were marginalized onto little mommy tracks and women had to be tough and strong and smart and so much better than their infantile male cohorts just for the outside distant small chance to be considered maybe almost equal. Asking a doc to reflect upon himself is akin to asking a politician to do the same, to reflect on massive bribery boozing drugs womanizing whores interns&gays. Therefore, encourage he Deelshad Joomun, MD s amongst us to find the sympathetic mind, regain awareness and position and family and friends, listen stand and speak with friends and peers, and for the colleagues and friends and peers and family to be aware and to pay attention and reach out with open arms to those desperate for help to rekindle or relight the warmth of life.
All it took for people to stop caring was 20-some years of someone else managing our care. We actually did it to ourselves. Because we wanted to “just” practice medicine, we gave all of our power away.
Take it from me: The mainstream media does not care about doctors done wrong – indeed, a major part of the political “playbook” used to get the ACA passed was demonizing physicians. In the current lexicon of the American press, doctors-of-all-specialties fit into one giant garbage can of social turpitude . . . we are all “rich” and “greedy”.
So no one cares now when our dreams are shattered and we die from a broken heart.
I get NYC news every day, where “if it bleeds it leads” rules the industry. It’s now Feb. 2, but not one word about this on any of the channels. Is this why Grey’s Anatomy ran the show on Dr. Bailey’s heart attack? This is simply not acceptable. What can we do to help?
This death is tragic, the high suicide rate amongst physicians is tragic. The health system employing this young doctor should perform a root cause analysis to this event, using this to inspire change in areas deemed lacking.
Unfortunately, there are many painful aspects to life, and we don’t know what plagued this beautiful soul. Facts are needed. Our collective anger needs to be focused on the proper issues. Focusing solely on the medical training environment may be premature, and it may not be the problem that needs to be corrected.
Facts are needed.
Dr. Hellman,
I respect your comment, however as a fellow physician who has been watching this movement grow,I can tell you with confidence that medical training is part of the problem. We are taught to suck it up and keep it to ourselves. Additionally, when we get out of training, we continue to live and work without the ability to reach out for help because the Board may hear of it and end the career we have already given so much for.
We isolate out of fear. If your patient were depressed you would recommend therapy and possibly medication. Why are doctors expected to shoulder the difficult issues of life and death for others and have nowhere to turn for help and support.
This needs to change! We have lost too many of our colleagues already!
I have to agree with your comment, seen so many broken ones, lose weight, stop in between patients and cry and pick up leftover food from patients trays to make it through the day. many come from other states, countries, no family around and expected to function at a specific level. it’s not easy for them. ????
The root cause has been analyzed. It is not one thing. Organizations that take away autonomy and break the psychological contract between organizations and clinicians and also between physicians and patients when they dictate care are part of the cause contribute greatly to the problem.
It is also fueled by lack of resilience–not in a “suck it up” way. I’m referring to how to properly manage stress and regulate emotions in a healthy way. In 2007, the actual definition of the purpose and use of emotions, knowledge that would greatly reduce stress physicians feel if they understood it and how to apply it, changed significantly. Prior to 2007, researchers would say, “We don’t know why humans evolved with emotions.” The new definition of the purpose and use of emotions is a game changer. Yet, because of the profit pathways that fuel new technology and Rx and lack of a clear pathway for new knowledge, the knowledge isn’t reaching people it could help. “Every two days now we create as much information as we did from the dawn of civilization up until 2003, according to Eric Schmidt, Google CEO, 2010”
Some of that knowledge could save lives. When I wrote my book on clinician burnout, I read over 500 published journal articles relating to burnout. That was on top of over 5,000 other journal articles I’d already read. Burnout has been studied.
One of the problems is the silos where research is being done. There is so much information in each silo that someone in a silo doesn’t know what someone else is doing that is related to their work. Almost no one is looking into a lot of different silos and seeing the big picture. They don’t know how the pieces of the puzzle fit together. Different words are used in different silos for similar concepts. For example, grit, hardiness, and resilience are used in different silos but they are closely related. Years ago, when I first began researching resilience I thought I’d pulled all the research I could find in the search engine. Then I stumbled across the use of the term hardiness in another silo and found nearly as much work in that arena as I’d found using the term resilience.
We also talk about and name high-level psychological concepts associated with beneficial psychological traits without relating them to the lower level concepts that they encompass–the lower-level concepts overlap significantly which clearly points to the solutions on the individual side since those beneficial traits can be developed.
The same information also points to solutions for adminstrators and patients. Greed is not a characteristic of someone who knows how to manage their emotions and stress to a good point. Greed and the strategies employed by many organizations reflect their own lack of ability to manage their own emotions. Incivil behaviors are indicators of poor emotion regulation skill and stress management. The research is clear that people who are skilled emotion regulators treat others better. Essentially, happy people are kinder, even to strangers, they aren’t committing crimes, and they display better corporate citizenship. Happiness is a reflection of low stress.
Our emotions are indicators that let us know how stressed we are. That is their purpose. Just like the purpose of hunger is to let us know it is time to eat and sleepiness lets us know it is time to rest our body, negative emotion indicates it is time to change something. Most often, in modern life, the thing that needs to change is perception which brings us around to psychological flexiblity and the new definition of emotions. Before the new definition of emotions many people second guessed the right thing to do, the right words to say, the right way to be. Emotions are indicators that let us know, in response to every thought we think, whether the thought is leading us toward self-actualization or away. When we are self-depreciating, it is away. When this is understood and practiced, it is possible to mentally navigate away from stressful thoughts and thoughts that lead bright young people (and others) to suicide. When we are self-compassionate, we are moving toward self-actualization.
Stress negatively impacts every aspect of our lives: physical health, mental health, relationships, cognitive ability, and central nervous system. Our digestive and immune systems do not function as well when we are stressed. We do not think clearly and we focus on problems instead of solutions when we are stressed.
Whether we believe we are good at managing stress or we believe we are not good at managing stress matters. The new definition of emotions will guide clinicians to more empowered mindsets and away from thoughts that lead to suicide. Once the new definition is understood, the thoughts that take us in the right direction are obvious–it is no longer guesswork!
Many of the physicians I meet with have developed something very similar to what Martin E. P. Seligman refers to as learned helplessness. Learned helplessness does not have to be pervasive–it can be subject specific. It is reversible. Understanding the new definition of emotions and how to apply it will reverse it because learned helplessness is an abject state of feeling unempowered. Our emotions guide us toward empowered mindsets because they are less stressful.
Feeling unempowered means they don’t feel free to push back against the stressors that are literally killing physicians. They might as well be chained like captives as long as they feel disempowered. They are like the circus elephant who doesn’t realize that he has the ability to break free from that rope.
Medical school does a job on them and then they go into employee situations that continue the process. It can be changed. The low-hanging fruit is helping doctors understand how to feel empowered. From there, from an empowered mindset, the solutions will flow because empowered mindsets see the bigger picture and focus on solutions.
I am sick and tired of these tragic preventable deaths. It is wrong that we do not have a clear path to bring information that has the power to save lives to people when it is created in research. To raise awareness about this issue I am walking from Santa Clara, California to Charleston, South Carolina in 2019. The same information that can empower and save clinicians can save at-risk children. Today we lose 2/3 of them to death, addictions, and prison. When knowledge about the root cause of human thriving becomes known, there is a moral duty to share that information with as many people as possible, as fast as possible.
Jeanine, I admire your commitment to thoroughly research a topic. You must be very-well acquainted with patience and persistence. My initial thought response to your ideas was one word – HAPPINESS. Although subjective and based on personal meaning, happiness is an all-encompassing emotion that can propel us toward or away from our over-arching goals in life. I will surmise that all people seek to be happy.
When we are less happy, we may not question why or take steps to improve our plight. We may not trust our ability and skill to change what we can or release our grip on what we cannot control. We may be afraid to navigate uncharted waters for fear of getting forever “lost at sea.” We may find it difficult to win back (willing gave away or taken from us) authentic happiness, but not an impossible result once we stay steadfast under the pressure of change. It is meant to refine us, but not to destroy us in the process. Have heart. No one fights alone. We are better together. Allow courage to lead us “home.”
My heart breaks for Deelshad and her family. May she rest in peace.
Very sad. We will be praying for her relatives and immediate family.
Thank you Dr. Wible for organizing this memorial to a beautiful, talented healer. She excelled at every opportunity in her life, and moved a half-world away to develop her skills even more, while taking care of so many. I did not know her, but I attended last night to show her friends and her family from afar that her life mattered, she touched us, and she will not be forgotten. I truly hope the ceremony and the dialogue afterward provided some comfort to the doctors and nurses there who lost their colleague.
what value life? the life of a hu-man animal or any other animal and plant life? we do not appreciate the precious tenuous nature of nature of life. rather we denigrate devalue what is different professing its badness and the need to torture it to kill it. difference is neither good nor bad but an opportunity to learn and to teach. the one ongoing forever task from the gods of its fantasy is to improve the speed and the efficiency of the kill. and that is the history of humanity, not hu-wo-manity. women are the brains and the sanity of the human creature race. we are slow to appreciate life as we deny the cheapness of life. this is more obvious in more cultures societies than not. there are no guarantees other than there is a beginning and an end. by the time we are aware there was a beginning, never mind, while the ending is at a time and place unknown, unless we choose to claim that power over life. knowing this history (not herstory) we cannot be surprised or shocked at how hu-mans torture and kill all life; doing so must be lots of fun since that is the history of man. considering how we treat the life of another, we cannot be surprised how badly we treat other life. obviously by destroying life we are destroying ourselves as we cannot remain on this planet without this planet. Live long and prosper image of Sarak. Live Love Laugh. Visit Neverland everyday, then go home; maintain reality and sanity. end of rambling.
Beautifully said Pamela <3 We will fight together to spread compassion from within. Thank you so much for being the gatekeeper for all these suffering souls. much love xo
Crisis interventions exists. If you are suicidal reach or to a mental health professional or colleauge who can connect you. Also 1800 lifenet and texting start to 741741 connects you to the crisis text line. Help helps. Reach out.
It is time for the wise, experienced but tired and abused healers to rise to the duty of healing doctors, medicine, our communities and our world. We have been cowed into silence, often brutally cowed, for far too long. Bad things grow in the darkness, in the silence. Reach out and talk with each other. Share your dreams, your challenges, your love for one another. Your love of your professional dreams, your patients. Say no. Regain control of your life and your happiness. That is the path to healing our community of healers.
I work 10 blocks away and NEVER ever heard of this happening. RIP dear doctor
How can we honor the life of our doctor if her death is covered up? So upsetting. It feels as if her very existence—that she every lived and walked on this planet—is being erased.
I am heartbrtoken for a Doctor, a woman, a person I have not known. My prayers and hopes for understanding why this has happened, go out to all those who knew and loved and respected her. All of you need to know that your lives matter to us, the people you take such good and loving care of. You, Doctors, are our family, our friends, our loved ones, and we want you to respect YOUR lives, as we respect YOU.
This is very sad and my thought and prayers go out to her family and colleagues. That said, as a current resident in my last year of training I would like to know when you say, “Many die a direct result of their training—institutionalized cruelty with rampant human rights violations illegal in any other industry“ what the heck are you talking about??? Residency is challenging and hard but nowhere near a “human rights violation”. This suggests that as doctors we are doing this to each other. It’s hard to see people suffering, hurting, and dying but it’s part of the job and we are there to alleviate that for patients so it’s necessary that we must see it. Some of us may be ill-equipped to deal with the day-to-day psychological stress of practicing medicine – but that’s not the fault of anyone and programs have made huge efforts to be aware and watchful for signs of psych and toxic stress issues and offer services without judgment. The real avoidable stressors in Medicine are paperwork, red tape, business, and politics – still hardly human rights violations and it’s inappropriate to use that term when there are real human rights violations happening in this world. I see your name more and more associated with these tragic cases and I’m curious, how long has it been since you even worked in an “institutional” setting? You seem to be completely out of touch with the reality of training today.
Institutionalized cruelty with rampant human rights violations illegal in any other industry:
1) Extreme and inhumane sleep deprivation:
Physician whistleblower exposes human rights abuse in U.S. hospitals
Sleep-deprived docs disclose hospital horrors
2) Bullying, hazing, sexual harassment & more:
Doctors-in-training hit with knives, punched, left crying in hospitals
3) Punished when sick:
Doctors-in-training punished when sick
I run a suicide hotline for doctors & med students and I am on the phone with these folks daily and they tell me EXACTLY what is going on in medical training today. That is the reality. I am not at all out of touch.
I’ve come upon your story via a Facebook post by a friend. I hope these tragic deaths, along with your heartfelt blog post serve as a wake-up call. If someone runs a medical school, what are maybe the top 5-10 things they could do to improve the experience of doctors and medical students. I thought about going to med school once, but once I learned about the sleep schedules, I decided against it.
Solutions outlined here: https://www.idealmedicalcare.org/blog/physician-suicide-101-secrets-lies-solutions/
I’m a PGY3. You must have a sweet residency or be in complete denial. Never had more than 12-hour shifts? Never had more patients than you could handle? Never had sicker patients than you could handle? Never made to go without food 24+hrs at a time? Never killed someone because you were left unsupervised?
You say that “some of us may be ill-equipped” to “deal” with our jobs. Are you just blaming the victims? I could easily say that if anyone succeeds in this type of environment that such a person is broken and unnaturally accustomed to suffering and incapable of functioning as a human being.
Your program has a “support system “? Interesting. Where are you training? What specialty? I’d love to switch!
Yes, Please do share ATMD. Love to know the stellar programs that support their residents.
I’m at UTHSC in Memphis, TN where I am a PGY4 in the Meds/Peds program. I’ve never been deprived of food for 24 hours and I have worked up to 28 hours at a time and *gasp* it was no big deal. I’ve never killed a patient and I have had supportive and available attendings. Reaching help has always been as simple as calling someone on my cell phone. We are busy and we work hard but we aren’t being tortured or abused. We are learning to be good doctors here and doing so safely and in an appropriate manner. To the PGY3 who commented above, if you think 12-hour shifts are a human rights violation then you don’t need to be working in medicine at all because even nurses work longer shifts and it’s been shown to be safer for patients. I worked longer and harder hours as a waitress. Some people actually have it harder than us and I for one appreciate the PRIVILEGE of being a resident.
To be clear, I have heard of an attending losing their temper and acting inappropriately and it was addressed swiftly and appropriately. I also have seen a restaurant manager yelling, bullying and throwing things at employees. This is part of being human and physicians are no exception but again, this is not behavior that is tolerated here.
Well, ATMD, you are lucky for having a supportive environment which is the exception not the norm. I really did not appreciate your sarcastic tone so right back at you. Your comments actually are part of the problem-the failure of those in the profession to honestly acknowledge what is going on. Just because you don’t want to cover up the fact that you are working over 80 hours a week, being paid seriously low wages while doing it, and then being asked to provide care for someone’s life is ridiculous and actually narcissistic. Your reference to waitressing is comical-I hardly see many waitresses committing suicide and serving someone a meal is a bit different than caring for a seriously ill patient. You can learn to be a great doctor without having to perform under these type of conditions. It makes me think that you didn’t even read the article and are totally unaware of what is really going on in the profession. Maybe you just don’t have the time…hmm.
Maybe you should consider yourself very fortunate that you’ve not experienced the horrors others have. And maybe your location and other factors at your specific site has something to do with not experiencing the exact pain that others have. But maybe you should step back and try to listen to what other people are experiencing and understand that you don’t speak for all doctors and residents or know everything about what’s going on. Having to work the crazy amount of hours past the legal threshold is most definitely a human rights violation, just one amongst others. The fact that it’s so regular doesn’t make it ok!
Doctors and medical students deserve the same legal protections that all others enjoy in the USA. Yet we are exempt from protection under ADA, HIPPA, labor laws that apply to every other industry. Enough excuses. These are human rights violations.
and yet, I don’t know of any program that offers these doctors a nurturing place to go have their souls taken care of. i have seen other doctors publicly shred the new interns to pieces, many in front of their patients, lot of them new to this country. Something nerds to be done to stop this cycle. Nurses need to also me more sensitive , its not an easy environment when all we do is take of others and not take care of each other … RIP to this beautiful soul ????
I reposted your blog on my page two days ago. It shook me, because her face is glowing with gentle hopefulness that you just want to bottle up and sprinkle over the world; Two,I live on the east side of the city, not too far from where this happened; and three,I had similar sentiments as a medical student. I had to find my own way, and luckily I did, though it was not easy, and I felt like I was in a constant wrestling match with my ego and need for approval. My inability to express “weakness” and ask for help turned into a giant snowball of disaster that threw me into the arms of a homeless, dangerous madman. Literally. And even now when I write about it, I have to ask myself, “Did that really happen?” because it still shocks and scares me. But with the wrong circumstances in place, the mind, anyone’s mind,can go to terrible places. Doctors are not immune; doctors are humans after all. Coincidentally, my experience will be published in the next week or two in a book I titled Manic Kingdom. But that’s not the point I want to make. The point I want to make is that I shared your blog post two days ago on my Facebook page, and after another quick search, there is nothing in the mainstream media about this? What?! I read above comments suggesting a cover-up of some sort? Would the hospital do that to protect its reputation? Or could this be cultural? You know, there is this feeling of being utterly trapped once you are in the trenches of med training- like you are stuck, and that breeds a dangerous level of hopelessness. You feel absolutely alone. Not talking about these occurrences and pretending like nothing is wrong, from the top down, only makes it worse. We need to share more stories and show people that they are not alone; that their thoughts are not silos and that it’s okay to feel sad, scared, anxious and depressed. Institutions need to be open and stop putting their reputations over the wellbeing of their doctors. People above stated that more professional mental health should be available to doctors. I agree, but also, on the grass roots/ peer level, much more can be done. The success and appeal of long-lasting, peer-run groups, like AA, are their ability to bring like-minded people together and share their struggles in a safe space.
Pardon the vent and very sad to see her go. May she rest in peace.
Coverups at every angle. From media (restricted by antiquated suicide reporting guidelines), medical institutions that should be holding morbidity and mortality conferences to investigate each case, families that have actually asked me to lie about the cause of death and cover it up after it has already been reported, religions that suggest you burn in hell for suicide. . . the list goes on . . . in 2018!
You are right that sharing these stories is essential. Sharing the truth. Honoring our beloved doctors (and others) we have lost to suicide. Not hiding them in body bags at private funerals.
Thank you for being so forthright and I can’t wait to read more of what you’ve written. Keep talking. Keep writing. Keep sharing. I am so glad you survived to tell your story.
The media is not restricted. The International Suicide Reporting Guidelines, which are not antiquated, are still often not followed despite knowing that when they aren’t it can lead to increased suicides because suicide can be contagious. But suicides can be and often are reported. If the media is not covering this it is because it doesn’t fit their narrative–not because of restrictions, at least not in the USA.
They can report who, when, and the occupation under the guidelines and they can report the prevalence which is the real story. Clinician burnout is the biggest threat to the healthcare industry. The lack of reporting is because they want to focus elsewhere.
The guidelines suggest not reporting the how because it increases suicide contagion.
The guidelines also suggest that every article about suicide provide the suicide prevention hotline number in case someone who is suicidal reads it.
What media restrictions are you referring to? The guidelines are suggestions, not mandated. They were developed by an international commission using evidence-based data. They are designed to prevent suicides.
Agree that there is lack of coverage for a variety or reasons including the taboo nature of the topic of doctor suicide and suicide in general. Seems some powers-that-be (those that own media channels) filter in and out stories depending on their overarching agends.
Yes, ratings. They should be all over this. Did you read the book, Bias? It was about the media’s quest for ratings and demonstrates that they don’t seek to inform–just to get ratings.
I recall in nursing school the saying that “nurses eat their young” I’m sure it is even worse with physicians. I am just baffled how this continues to be the climate in the medical field. This is a step towards breaking that cycle. We can try and just blame the industry, but it’s the people in the industry that allow it to grow and fester into this toxic and sometimes deadly environment.
I just wanted to thank you for your post about my friend Deel who sadly took her own life. I was an intern with Deel at Pennsylvania Hospital from 2011-2012. She was well liked by all those who came into contact with her. She will be remembered for her kind and warm personality. The photograph of her looking upwards almost captures her spirit as I remember it.
Mental health among physicians has long been ignored and I appreciate your post about this important issue.
I get NYC news every day, where “if it bleeds it leads” rules the industry. It’s now Feb. 2, but not one word about this on any of the channels. Is this why Grey’s Anatomy ran the show on Dr. Bailey’s heart attack? This is simply not acceptable. What can we do to help?
Contact news media. There is a long history of covering up these suicides.
From her picture, one can see the beautiful person Deelshad physically as well as personality. Her face reflects her name “Happy Heart.” Now the world is that much darker as this physician who would have changed the lives of many patients for the better has extinguished her light because of medicine’s culture. Physicians and those in- training maintain their human frailities as they travel the rigourous journey to their dream of helping others. Administrators, Attendings, Faculty and everyone else involved in their training need to change their focus from tearing down these healers to building up their confidence and psyche as well as their knowledge. Heaven has gained a new angel. RIP Deelshad <3
for people like ATMD who may be experiencing privilege and are untouched by the horrible circumstances which are a norm for many/most residents and even attendings, i’m glad you have it good congrats. go on in your bubble if you’d like 😉 . but at least pretend to have some empathy and understanding (aren’t you a doctor?) for your colleagues while the rest of us work towards fixing the problem. when people are routinely jumping off of buildings from the same institution it becomes quite clear there is a larger and deeper issue.
“Human rights are moral principles or norms[1] that describe certain standards of human behaviour, and are regularly protected as legal rights in municipal and international law.[2] They are commonly understood as inalienable[3] fundamental rights “to which a person is inherently entitled simply because she or he is a human being”,[4] and which are “inherent in all human beings”[5] regardless of their nation, location, language, religion, ethnic origin or any other status.[3] They are applicable everywhere and at every time in the sense of being universal,[1] and they are egalitarian in the sense of being the same for everyone.[3] They are regarded as requiring empathy and the rule of law[6] and imposing an obligation on persons to respect the human rights of others,[1][3] and it is generally considered that they should not be taken away except as a result of due process based on specific circumstances;[3] for example, human rights may include freedom from unlawful imprisonment, torture and execution.[7]”
1. is it considered a norm for people to kill themselves in their workplace? didn’t think so either.
2. the cases of the two women at Sinai would have gone ignored if it weren’t for dr. wible.
3. these human rights violations are driven by corporate greed, politics etc
(Hug) for all touched by the tragic death of Deelshad, MD.
NOW, not later or never, is the time for all health systems to quit burying their heads in the sand by denying a problem of suicide exists in their respective institutions. My hope is for one brave health system, including their stakeholders, to get in contact with you, Dr. Wible, to invite you to round-table discussions on Best practices of ideal medical care and the grave topic of suicide. NOW is no time for health systems to fear improving systemic quality of life for ALL. NOW is the time rise above ignorance. Brilliant management of health systems: Be a STAND-OUT institution for positive social change. Partner with Dr. Wible NOW! Character and integrity is better than reputation.
Information and advice = Prevention. And even an ounce of prevention is better than practicing no prevention at all.
Establishing, running and maintaining a residency program can be compared to running a successful business. There is money poured into it and there is money expected to be reaped back from it. Everything from getting an interview, hiring process, the voting, the second look, the “match”, “soap” all of these have been created to give a so called “transparency” to the process when it fact, it is well known that this is the most corrupt, maligned process created and controlled by few handful of physicians who can make or break your entire career with a single letter. The “fear” culture has been instilled from early on in medical school. Program directors are to be venerated as GOD next to program co-coordinators/older residents. Not to forget the pretentious smiles and gimmicks they all do at each residency fairs/interview dinners/post interview love notes before matching day. If someone dared to raise their concern, either resident or the faculty, they are shunned and cast out by the rest. I would compare modern day residency program to old school MAFIA system.Very few programs and physicians are out there that does it purely out of their love for medicine and teaching. Most people choose to suck up for few years and get out to real world.
So terribly sad. That we do this to each other. Physicians willing to prey on others who are struggling to maintain their dreams. We should support each others. A family atmosphere of acceptance and love. Even the military has this down: Medical student: “I was less stressed in Afghanistan”
Regarding the latest article: Why Do Female Physicians Keep Dying By Suicide At This Hospital?
A Culture Of Silence
In an initial email following the death, which occurred on Thursday evening, the hospital’s administration sent a curt and impersonal note to its staff. “I am writing to inform you that a former tenant at 515 West 59th Street, a Mount Sinai-owned residential building, was found dead there earlier today, possibly a suicide,” the email said. “The NYPD are investigating, and as soon as we learn more details we will inform you.”
Without any confirmation about who had jumped from the building, residents were left to whisper through the halls of the hospital in an effort to piece together what happened. One told Refinery29 she was in a group chat with other residents, trying to confirm they were all accounted for.
Several said they only found out about the incident through word of mouth or by coming home to see police tape and a body bag in front of their building.
The next morning, before sending a formal message announcing Dr. Joomun’s death and offering condolences, the administration sent an email reminding staff of the hospital’s media policy. (A Mount Sinai St. Luke’s spokeswoman said that the hospital media policy is “general” and that she couldn’t recall an email about the policy being sent out following the suicide.) Refinery29 reviewed the email and confirmed it was sent the morning after Dr. Joomun’s death.
“Please take a moment to review Mount Sinai Health System’s policies surrounding Press and Media inquiries and Social Media policies. It is very important that all faculty, staff, and students understand these policies and adhere to them,” the email, obtained by Refinery29, read. “Do not respond or speak to any reporters, as well as current or former employees, regarding a pending news story.”
Then, the administration sent a third email: “It is with sadness that we share with you the news of a tragic loss of life of a member of the Department of Medicine faculty (with a secondary appointment in Radiology) at Mount Sinai St. Luke’s and Mount Sinai West. We are not providing further details out of respect for the family’s privacy.”
Facebook message I just received today (from Sinai med student who wishes to remain anonymous for fear of retribution): Dr. Wible, Id like to thank you for covering the story about the Dr.Deelshad Joomun. I am a student at Icahn School of Medicine at Mount Sinai. As I read your article, I was surprised that they don’t “recall” the email sent about media policy. I just checked my school email, and they sent the email regarding the suicide at 10:21 am, and a couple of seconds later they also sent an email titled “press and social media inquiries and social media policies”. I just wanted to verify that In fact, that email does exist. Thank you again for raising awareness.
May Her Memory Be a Blessing.
this is horrible and so sad. Why Sinai? Is it a stressful place to work at? Why women docs? Is it malignant toward women? this should be investigated further.
Yes full investigation required and long overdue.
This is so sad.I think that Doctors are some of the most hardest working health care professionals and the least respected ones.I worked in a institution where Nursing Assistants
would actually tell Doctors what to do.No respect and this is what brought on the demise of Beth Israel
Medical Center on 16th St and 1st Avenue.Everyone was a boss except
the Doctors
The attitude of condescension and lack of empathy expressed by ATMD truly is one of the most insidious obstacles we face in making meaningful change. I am also a resident in my final year of training, and have overall been blessed with a generally supportive program. I have worked many 28 hour shifts that were challenging but manageable, and I understand they exist for continuity of care. I have also almost fallen asleep behind the wheel after these shifts and struggled to maintain my sense of well-being after bearing witness to so much suffering and poverty (I am a resident at a county hospital- so many of my patients are fighting uphill battles and the injustice of it all has definitely worn on me throughout my training).
We have to recognize that this is a difficult job and it takes a lot of support and help to get through medical training, even under the best of circumstances. I deeply worry about colleagues who are not as fortunate and also have to deal with a toxic training environment. My heart breaks for my friends and colleagues who have lost residents and classmates to suicide. An institution not far from mine experienced the devastating loss of an intern at the beginning of the year, and it began to leak out from current residents that ongoing duty hours violations and mistreatment by Attendings are rampant at this program.
We have to take care of one another. We have to stand up for each other as a group and say we will do what it takes to put a stop to physician suicide, and that includes admitting that human rights violations absolutely do happen, even if they are not happening to us. Please, don’t trivialize the suffering of others. That is not the mark of a physician.